Closed-Loop Referral Tracking: Why Most Social Care Networks Still Fall Short
01 Jul
Key takeaways
- “Closed-loop” is widely misused. Confirming a referral was received is only the first of four steps before anything is actually resolved.
- NCCARE360 has the infrastructure. The gaps come from CBO documentation capacity, inconsistent outcome definitions across partners, and missing EHR connectivity on the return journey.
- Switching platforms does not fix this. Every major social care network has the same structural gaps because the problem is how data flows between systems, not which system is being used.
- FHIR R4’s ServiceRequest and Task resources were built specifically for this workflow. A FHIR facade layer can route structured status updates from CBOs into existing clinical systems without touching current workflows on either side.
- Before any technical fix works, CBO partners need to agree on a shared outcome taxonomy. The Gravity Project’s SDOH value sets give networks a ready-made framework to work from.
Closed-Loop Referral Tracking: What It Means, Why Most Social Care Networks
Do Not Have It ?
A patient presents for a follow-up appointment and the care manager asks if they connected with the housing navigator from three weeks ago. The patient has never heard of him. The care manager checks the system and finds a status that reads “Referral sent,” nothing more.
No acknowledgment from the destination agency. No record of whether anyone reached the patient. No indication of what, if anything, happened once the referral left the team’s hands.
If you manage a care coordination team, you know this scene well. Sending referrals is not the hard part. Any network handles that. The hard part is what comes after.
Table of contents
What a closed loop actually means
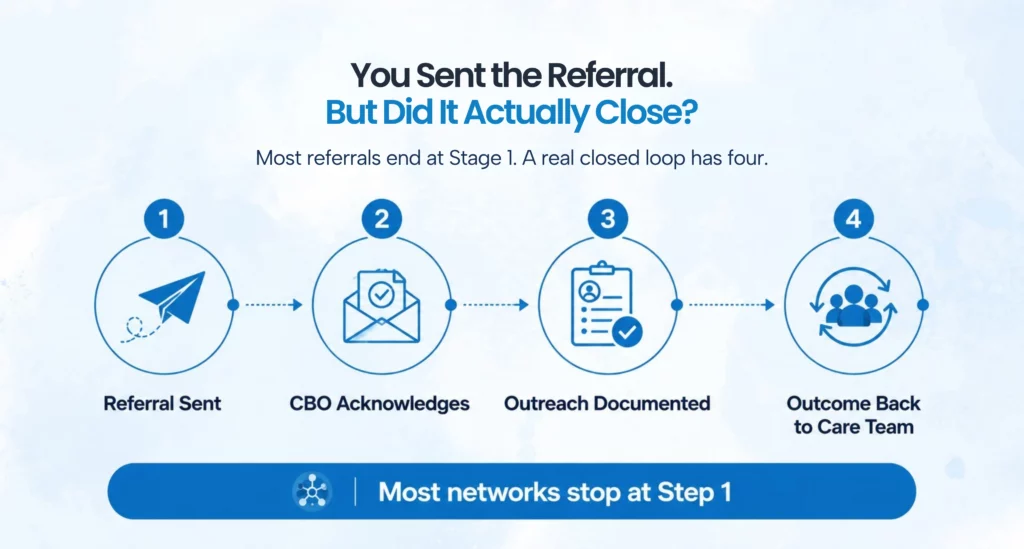
The term gets used loosely across social care, and that looseness creates a false sense of confidence about what systems are actually doing. Many platforms describe themselves as closed-loop because they can confirm a referral was received by the organization on the other end, but that is only the first stage of a process that requires four distinct steps before anything is actually resolved.
A true closed loop means the referring care team gets structured confirmation at every stage after the referral leaves their hands. The community-based organization acknowledges receipt, documents whether they were able to reach the patient and what happened during outreach, and then sends a final outcome status back to the care team in a specific, processable form, whether that is services delivered, patient declined, patient unreachable, or referral redirected elsewhere. That last stage is where nearly every social care network breaks down, and the result is a care team that has no idea what happened to a referral until the patient walks back in for a visit and admits they never heard from anyone.
Why NCCARE360 participants are still running into this
NCCARE360 is worth naming directly because it represents genuinely serious infrastructure. Launched in 2019 through a collaboration between the North Carolina Department of Health and Human Services and Unite Us, it spans thousands of organizations statewide and covers a wide range of social needs from housing and food access to transportation and utility assistance. Even with all of that in place, care coordination directors working inside NCCARE360 consistently report that referral outcome data does not reliably make it back to the clinical side in a usable form.
The reasons come from several directions at once, and none of them are solved by switching platforms. Community-based organizations are being asked to close the loop without the staffing capacity to do it consistently. Logging a structured outcome in the network platform for every referral received, often from dozens of different referring organizations across multiple systems, is a real documentation burden for a small nonprofit running on two staff members with a packed caseload. The fields exist in the platform, but the data frequently does not get entered because serving clients takes priority over updating a platform, and that is a funding and capacity problem that technology alone cannot fix.
Platform adoption across the network is also uneven, which has a direct impact on data quality. NCCARE360 works well when every party in a referral pathway is actively using it, but when a CBO accesses the network infrequently or logs outcomes several days after the fact, real-time status tracking becomes unrealistic regardless of what the platform technically supports. There is also no agreed definition of what “resolved” means across partner organizations, which matters more than most people realize. One CBO marks a referral closed when services are delivered, another marks it closed when the client declines, and a third marks it closed when outreach attempts have been exhausted. Those are three completely different outcomes with different implications for the care team, but they look identical inside a system that accepts free-text closure notes instead of standardized codes.
Even when a CBO does close a referral properly, that status rarely flows back to the referring provider’s EHR automatically. The care manager has to open a separate platform, locate the referral, read the status, and manually update the patient record. That two-step process is manageable in isolation, but it falls apart completely when a care manager is tracking open referrals across 80 or 90 active patients with multiple CBO partners in the mix.
What fixing this does not look like
Two approaches come up regularly in these conversations and are worth addressing directly before getting to what actually works. Switching to a different social care platform rarely solves anything because every major network has the same structural gaps, and those gaps exist not because of product failures but because of how data flows between systems and how outcome definitions are or are not standardized across partners. A different platform with the same underlying architecture produces the same results with a different login screen.
Hiring a dedicated referral coordinator to manually track loop closures is a short-term fix on a problem that gets harder as referral volume grows. The coordinator becomes the loop, and when their caseload fills or they leave the organization, the loop breaks again. It also does not produce the kind of structured, queryable data that would let a care coordination director understand how referral pathways are actually performing across the network.
How to close the loop without starting over
The referral outcome data exists somewhere in most cases. The problem is that it sits in the wrong system, arrives in a format that cannot be processed automatically, or requires manual steps that do not happen consistently enough to be reliable. Fixing it means changing how data moves between systems, not adding more people to move it manually.
Connecting the social care network to FHIR infrastructure is the most direct path to automated loop closure. FHIR R4 has defined resource types built specifically for this kind of workflow: the ServiceRequest resource captures the referral itself, and the Task resource tracks its status through each stage, from received and in-progress through to completed or failed. When a CBO updates a referral status in their platform, that update can be structured as a FHIR Task status change and transmitted automatically back to the referring organization’s clinical system, so the care manager sees the updated status in the tool they are already working in without opening a separate platform or waiting for a phone call. FHIR R4 has supported this pattern since 2019, which means the gap is not the standard itself but the missing interoperability layer between systems that should already be exchanging this data.
Before any of that can work reliably, the outcome taxonomy question has to be resolved with CBO partners. The Gravity Project has developed standardized SDOH value sets that define exactly how social needs and referral outcomes should be coded in FHIR, covering housing instability, food insecurity, transportation barriers, and other categories with specific codes for each outcome type. When all partner organizations are working from the same taxonomy, the status that returns from a CBO is structured and processable rather than a free-text note that requires human interpretation before it can inform a care decision. This conversation with CBO partners typically takes one structured meeting to work through, and it makes every downstream technical improvement significantly more reliable.
Once the data is structured and flowing, care managers need to receive status updates as triggered alerts inside existing tools, not as passive notifications in a platform they check when they remember to. When a referral closes without services delivered, the care manager needs to know that the same day, not at the patient’s next scheduled visit. Structured FHIR data can trigger those alerts through existing EHR notification frameworks without custom development, because the infrastructure is already built into most clinical systems and just needs incoming data in a readable format.
What becomes measurable when the loop actually closes
Most care coordination teams do not have access to the following metrics today, not because they are complicated to track but because the underlying data is not structured or centralized enough to surface them without significant manual effort. When the data architecture is working correctly, these numbers become visible without adding any new manual tracking steps to the team’s workflow.
Referral acknowledgment rate shows what percentage of referrals sent receive structured confirmation from the receiving CBO within a defined window, typically 48 to 72 hours. Outreach completion rate shows how many acknowledged referrals document at least one contact attempt with the patient. Loop closure rate by CBO partner is where capacity gaps and training needs tend to show up most clearly, because the variation across partners is almost always larger than care coordination directors expect before they can actually see the numbers. Time to closure shows how long the average referral takes to reach a documented outcome, and referrals aging past 30 days without a status update almost always point to a specific breakdown in the workflow rather than a general slowness across the board.

Where to start if you are inside NCCARE360
Most care coordination directors who get to this point in the conversation ask the same question: where do we actually begin? The honest answer is that the starting point is not a technology decision. It is a diagnostic one. Before connecting anything or changing any workflow, it is worth mapping exactly where the loop breaks for your specific organization, because the failure point is rarely the same in every network and every partnership mix.
For most NCCARE360 participants, the referral sending side works. The relationships with CBO partners exist. The harder question is what happens after the referral leaves the care team’s hands and whether that return journey, the status updates, the outreach records, the outcome data, is reaching the clinical side in a form the team can actually work with. Often it is not, and the gap is somewhere in the translation between systems rather than in anyone’s intentions.
Once that gap is identified, the fix tends to be more contained than it looks from the outside. A FHIR-based interoperability layer connecting NCCARE360 data to existing clinical systems can bring structured status updates into care management workflows without rebuilding platforms or retraining staff on new tools. The care team keeps working the way they work. The CBO partners keep working the way they work. The difference is that the outcome data travels to where it needs to be, automatically, and the care manager is not left wondering what happened to a referral sent three weeks ago.
That is ultimately what closing the loop is about. Not the technology, not the compliance checkbox, but the patient who showed up for a follow-up visit and actually received the help they were referred for, and the care team that knew about it in time to make a difference.

FAQs
It means the care team that sent the referral receives confirmation of what happened at every stage after it left their hands: whether the CBO received it, whether they reached the patient, and what the final outcome was. Most networks only confirm the referral was sent, which is just the starting point.
It is common across every major social care network. NCCARE360 is a serious and well-built network, but closed-loop gaps show up everywhere because the structural challenges, CBO documentation capacity, inconsistent outcome definitions, and missing EHR connectivity, are not unique to any one platform.
No. The fix is in the layer connecting those systems, not in the systems themselves. Organizations can keep their existing EHR and social care network while adding an interoperability layer that moves status data between them automatically.
It is a structured data object in FHIR R4 that tracks the status of an activity as it moves through a workflow. In a referral context, it carries status updates from the CBO back to the clinical system at each stage, without anyone needing to manually log in to a second platform to check.
It is a national initiative that defines standardized codes for social determinants of health data in FHIR. When organizations use Gravity-compliant codes for referral outcomes, the closure status that comes back from a CBO is structured and readable by clinical systems rather than being a free-text note that requires someone to interpret it.
Start by tracing one referral end to end: when was it sent, when was it acknowledged, when was the patient contacted, and when did a final status return to your team. For most organizations, the breakdown becomes obvious in that exercise, usually at the point where data needs to cross from the social care network into the EHR.
Categories
- 1115 Waiver (8)
- ACO (7)
- AI (30)
- Aigilx Health (30)
- CCBHC (8)
- Control Center (10)
- FHIR Facade (7)
- FHIR Server (14)
- HIE (5)
- Payers (8)
- Providers (11)
- Rapid Fire (9)
ISO 27001:2022 Certified
Aigilx health specializes in developing Interoperability solutions to create a healthcare ecosystem and aids in the delivery of efficient, patient-centric and population-focused healthcare.
