How to Automate Medicaid and MCO Reporting for Social Care Programs Without Rebuilding Your Data Infrastructure?
03 Jul

Key takeaways
- Medicaid and MCO reporting is manual because reporting requirements were written for clinical data systems, not the case management tools and CBO databases social care programs actually run on.
- Automation does not mean replacing existing platforms. A FHIR R4 interoperability layer connects what you already have to what funders need, without a data migration.
- Three data problems block automation before it starts: inconsistent member identifiers across systems, SDOH screenings captured as free text rather than coded values, and batch export processes too slow for monthly MCO submission cadences.
- Programs operating under state contracts like the NYS 1115 Waiver also need to handle inbound data from MCOs, not just outbound reports. An interoperability layer covers both directions.
- The organizations that get automated reporting working are the ones that fix data capture at the source first, before expecting any pipeline to clean it up on the way out.
How to Automate Medicaid and MCO Reporting for Social Care Programs Without Rebuilding Your Data Infrastructure?

Do Not Have It ?
It is the last week of the reporting cycle. Three staff have been pulled off their regular work to compile member activity logs, service delivery records, and SDOH screening data from four different systems. Someone is manually checking whether the MCO’s required fields match what the case management platform actually captures.
Someone else is reconciling member IDs that look slightly different across two data sources. A spreadsheet that started as a template is now forty columns wide and no one is entirely sure it is right.
This is not a story about a disorganized team. It is what happens when reporting requirements were designed for one kind of data system and the organizations doing the work are running on a different kind entirely.
Table of contents
Why reporting keeps getting harder
The underlying tension is straightforward. Medicaid managed care contracts and MCO reporting requirements were largely written with clinical data systems in mind: structured records, standardized formats, clear encounter codes. Social care programs, by contrast, run on a very different mix of tools. Case management platforms, CBO databases, referral networks, screening tools, and spreadsheets all hold pieces of the data that funders want, but none of them were designed to talk to each other or to export in the format a Medicaid MCO expects.
The result is that reporting becomes a translation job on top of an already demanding operational workload. Staff pull raw data from each system, reformat it manually, check for missing values, reconcile member identifiers that do not match across platforms, and then hope the final file meets the MCO’s submission specifications. When a funder changes their data template, which happens more often than it should, the entire process starts over.
What makes this particularly draining is that the data itself usually exists. The screening was conducted, the referral was sent, the service was delivered, and someone logged it. The information is in the organization’s systems somewhere. The problem is getting it out in the right shape, at the right time, without requiring a team of people to do it by hand every single reporting period.
What automation actually means in this context
When operations directors hear “automate your reporting,” the instinct is often to assume it means a major IT project: new software, data migration, months of implementation, and a budget conversation nobody wants to have. That assumption is understandable but it is also what keeps most social care programs stuck in manual reporting cycles longer than they need to be.
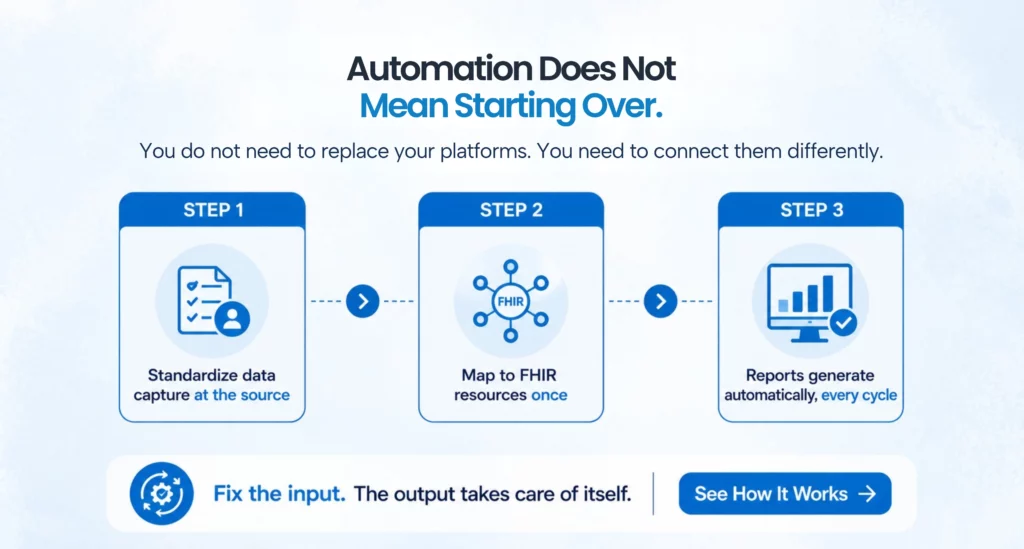
Automation in this context does not mean replacing your case management platform or your referral system. It means adding a layer that connects those existing systems to reporting outputs in a standardized, repeatable way. The data stays where it already lives. The automation layer handles the translation, the formatting, and the delivery.
The standard that makes this possible at scale is FHIR, specifically FHIR R4, which has defined structured resource types for exactly the kind of social care and SDOH data that Medicaid and MCO reports require. When social care data is mapped to FHIR resources, it becomes machine-readable in a format that multiple downstream systems, including MCO reporting portals and state Medicaid systems, can consume without manual reformatting. The mapping work happens once. After that, the report generation becomes a scheduled, automated process rather than a quarterly all-hands exercise.
Where the data problems actually live
Before any automation can work reliably, it helps to understand exactly where the data quality and format problems are coming from, because they are not the same in every organization.
The most common issue is member identifier inconsistency. A Medicaid member might appear under their full legal name in one system, a nickname in another, and with a slightly different date of birth in a third. MCO reports require a single consistent identifier, usually the Medicaid ID, tied to every service record. When that identifier is missing or inconsistent across systems, reconciliation becomes manual by necessity. Automated reporting requires that member identifiers be standardized upstream, which means addressing how member data is captured and stored in each source system, not just how it is exported.
The third issue is timing. Many social care programs operate in a batch reporting world where data is pulled, cleaned, and submitted at the end of a reporting period. MCOs are increasingly expecting near-real-time data or at minimum monthly submissions with shorter lag times between service delivery and reporting. Batch processes built on manual exports cannot keep up with that cadence without adding staff. Automated reporting built on FHIR APIs can.
What a realistic automation path looks like
The path to automated Medicaid and MCO reporting does not require replacing existing systems. It requires connecting them differently and standardizing how data enters them at the source.
The starting point is an honest audit of current data sources. Which systems hold the data your MCO reports require? How is member identification handled across those systems? Are SDOH screenings captured as coded values or as narrative notes? Where are the gaps between what you currently collect and what reporting templates require? This audit does not need to be a months-long project. Most operations directors can get through it in a few weeks with the right framework.
Once the gaps are mapped, the next step is standardizing data capture at the source. This means working with the teams using case management and screening tools to ensure that the fields MCO reports rely on are being filled consistently and in a format that can be mapped to FHIR. This is a workflow change, not a technology change, and it is the step that most automation projects skip, which is why they fail. Automation that runs on poorly structured input data produces poorly structured output data, and that does not pass MCO validation.
With clean, consistently structured data coming in, a FHIR-based interoperability layer can then connect source systems to reporting outputs automatically. FHIR ServiceRequest and Observation resources handle social care service records and SDOH screening results respectively. FHIR Patient resources carry the member demographic and identifier data MCO reports require. When these resources are populated from source system data on a scheduled basis, report generation becomes a matter of querying those resources and formatting the output to match the MCO’s submission template, rather than pulling raw data from four different platforms and reformatting it by hand.
For organizations operating under specific state programs like the NYS 1115 Waiver, FHIR-based reporting automation also addresses the bidirectional data exchange requirements that those contracts include. Reporting is not just outbound in those contexts. MCOs and state agencies are also sending back member eligibility updates, care plan changes, and service authorizations that social care programs need to receive and act on. An interoperability layer that handles both directions removes a second set of manual processes that most programs are currently managing through email and fax.
What changes operationally when reporting is automated
The most immediate change is time. Operations directors who have been spending two to three weeks per quarter on report preparation typically see that compress to a few days once automated pipelines are in place, because the data is already structured and the formatting is handled by the system rather than by staff. That time goes back into program work.
The second change is accuracy. Manual report compilation introduces errors at every hand-off point: the staff member who exports the wrong date range, the spreadsheet formula that references the wrong column, the member ID that gets transposed. Automated pipelines with validation rules catch those errors before submission rather than after an MCO kicks back a report for resubmission.
The third change is auditability. When reporting runs through an automated pipeline, every step of the process is logged. Which data source fed which field, when the report was generated, what validation rules ran and what they flagged. That audit trail is something most social care programs currently cannot produce when a funder asks how a number was derived, and it is becoming more important as MCO contract oversight tightens.
Where to start without overwhelming the team
The mistake most operations directors make when approaching this is trying to automate everything at once. Choosing one MCO report as a pilot, mapping its required fields against current data sources, fixing the data quality issues in those specific fields, and building the automation pipeline for that single report is a more manageable path. Once that pipeline is running reliably, expanding to other reports or other funders is largely a matter of adding new output templates rather than rebuilding the underlying data architecture.
The organizations that have made the most progress on this are not necessarily the ones with the largest budgets or the most sophisticated technology teams. They are the ones that treated data quality as a prerequisite rather than an afterthought, that standardized how SDOH and service data is captured before expecting automation to handle the rest, and that chose an interoperability approach built on open standards rather than proprietary integrations that require renegotiation every time a funder changes their template.
That foundation is what makes reporting repeatable, auditable, and sustainable across multiple funders and multiple reporting cycles, without adding headcount every time a new requirement comes in.


FAQs
Social care programs typically run on case management tools, referral networks, and screening platforms that were not designed to export data in the structured formats Medicaid and MCO contracts require. The data exists, but getting it into the right shape for submission becomes a manual translation process that repeats every reporting cycle.
No. Automation means adding an interoperability layer that connects your existing systems to reporting outputs in a standardized format. Your case management platform, referral network, and EHR remain in place while the integration handles data transformation automatically.
FHIR R4 is a healthcare data standard that defines structured resource types for clinical and social care information. When social care data is mapped to FHIR resources, it becomes machine-readable and can be submitted to Medicaid agencies and MCO reporting systems without repeated manual reformatting.
The Gravity Project develops standardized FHIR-compliant codes for social determinants of health (SDOH) data. Capturing screening results with Gravity-aligned codes ensures they are already structured for automated Medicaid and MCO reporting instead of requiring manual interpretation from free-text documentation.
Organizations should standardize on a single member identifier, typically the Medicaid ID, across all source systems. Establishing this common identifier through data governance is essential before automation can reliably match, reconcile, and report data across multiple platforms.
A pilot for a single Medicaid or MCO report typically takes six to twelve weeks. This includes assessing existing data, standardizing source systems, building the integration pipeline, and validating report outputs. Timelines vary based on the number of connected systems and overall data quality.
Categories
- 1115 Waiver (8)
- ACO (7)
- AI (25)
- Aigilx Health (25)
- CCBHC (8)
- Control Center (10)
- FHIR Facade (7)
- FHIR Server (14)
- HIE (5)
- Payers (8)
- Providers (11)
- Rapid Fire (9)
ISO 27001:2022 Certified
Aigilx health specializes in developing Interoperability solutions to create a healthcare ecosystem and aids in the delivery of efficient, patient-centric and population-focused healthcare.
